
Case Report | DOI: https://doi.org/10.31579/2578-8868/006
1 Department of Neurosurgery, University of the Witwatersrand, Johannesburg and Chris Hani Baragwanath academic hospital
*Corresponding Author: John r. ouma, Department of Neurosurgery, University of the Witwatersrand, Johannesburg and Chris Hani Baragwanath academic hospital ,
Citation: John r. Ouma, challenges in spinal care in sub-Saharan Africa (ssa) , J Neuroscience and Neurological Surgery. Doi: 10.31579/2578-8868/006
Copyright: © 2018 John r. Ouma fcs. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 06 March 2018 | Accepted: 30 March 2018 | Published: 06 April 2018
Keywords: Spinal cord injuries, Paraplegia, Tetraplegia, Wheelchair, Pressure ulcer
Spinal conditions are commonplace in the developing world, and Sub-saharan Africa (SSA) is no exception.
Traumatic conditions of the spine occur regularly, and when they do, they usually demand a level of urgency in diagnosis and treatment, not to mention skill on the part of the treating doctors. Tuberculosis of the spine as well as tumours and degenerative conditions are also big players in this arena.
Spine care is complicated by fact that spine instrumentation is technology and cost intensive, which does not sit well with many third world countries.
All these factors taken together create a hostile environment which leads to outcomes far from ideal for the spinal patient.
OBJECTIVES:
To describe the presentation and management of four patients from SSA countries presenting with spinal problems whose management illustrates some of the problems referenced above.
METHODS:
Discussion of four cases and review of the literature.
It is common cause that the state of health care in SSA lags far behind that of the other continents.
There are several political, social, historical and economic reasons why this is so.
Spine surgery is a complex area of medical practice. The requisite human resources, doctors and nurses tooled and resourced in spinal diagnosis and management, are few and very far between.
The equipment requirements are demanding, expensive and not easily available.
The SSA spinal patient finds himself immersed in this reality.
Other than locales in the north and south of the continent, this applies to much of Africa.
Spinal trauma is a common cause of patients presenting to neurosurgical units in these countries (1). In a study, Rabiu found this to be the case in a rural Nigerian tertiary hospital where trauma accounted for 68% of these patients (2).
This finding has been confirmed by other researchers, who have noted the prevalence of road traffic accidents as the main contributor to this scourge (3, 4).
Lumbar disc conditions as well as degenerative lumbar stenosis have been found to be the commonest cause for non-trauma neurosurgical consultations in SSA (5).
Doctors at the forefront of providing spinal care in SSA face many challenges. These include delayed presentation of patients, missed diagnoses due to poor radiological support or inability of patients to afford investigations, non-availability or sheer cost of required implants, as well as lack of suitable personnel and hospital equipment (3, 6, 7). Yet where efforts are made, despite lack of resources, some benefit can be achieved (5, 8).
One aspect of spinal care in SSA that has not been highlighted sufficiently in the past is the challenges faced when patients are transferred abroad for management, either de novo or after an initial attempt at surgical treatment in the base country.
This paper presents four such cases, each with a unique set of circumstances that highlight certain aspects of this problem.
Patient 1:
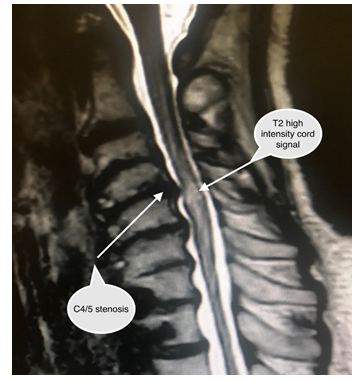
This lady presented to a spinal centre complaining of neck pain and progressive onset of numb, clumsy hands. She also had oncoming stiff legs and gait disturbance.
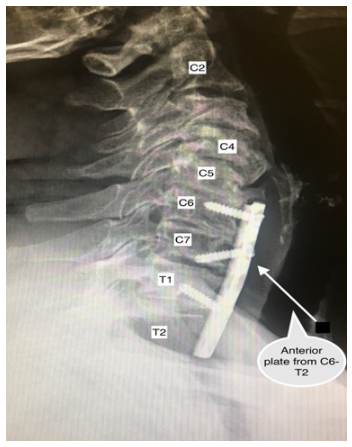
An MRI scan did show radiological findings consistent with cervical spondylotic myelopathy at the C4/5 level (Figure 1). Inexplicably, she was offered an anterior cervical plate from C6 to T1 (Figure 2) via a right sided approach. No intervertebral decompression was done at those levels and specifically not at the C3/4 level, where her pathology sat and therefore where treatment should have been rendered.
Unsurprisingly, she felt no better and sought further treatment in Johannesburg, where the pathologic level was addressed.
Patient 2:
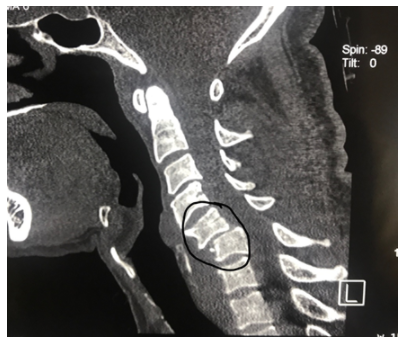
This patient presented with quadriparesis following a motor vehicle accident in which he sustained a bi-facet cervical dislocation at the C5/6 (Figure 3) level. Cones callipers were applied in an attempt at reduction; however, this was unsuccessful, not surprising seeing that the skin was lacerated at the application sites bilaterally (Figure 4), a tell-tale sign of improper calliper application. He was sent to Johannesburg three months later, the delay occasioned by financial and immigration issues, where a reduction and instrumented fusion were eventually done, with the expected degree of difficulty encountered in dealing with delayed facet dislocations.

Patient 3
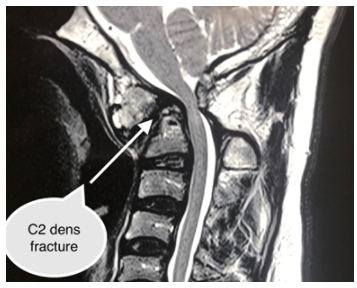
This patient was involved in a car accident some 11 years beforehand, and had always complained of neck pain right from the day of the accident. He had never been formally investigated till recently when he developed oncoming weakness of his hands and legs. A neglected fracture of C2 with anterior dislocation of the dens and severe stenosis of cervical cord was found (Figure 5). A posterior decompression and in situ occipito-cervical fusion was performed.
Patient 4
This patient was involved in a road traffic accident, developing severe neck pain directly thereafter. Scans showed a unifacet fracture dislocation and grade 1 anterolistheis at C6/7. She was treated conservatively for a year, and then eventually had a unilateral lateral mass screw placed between C5 and C7, in addition to spinal wiring at C3/4 (Figure 6). The reason for the wiring was difficult to follow, and the lateral mass screws were problematic; they were placed unilaterally, there was no attempt at reduction, and the trajectory of the lower screw was unusual and potentially dangerous, in that the path of the vertebral artery was disregarded in placing it (Figure 7). The implants were removed and a decompression and fusion at the affected level was performed.


These cases teach a number of lessons about the state of spine care in some parts of SSA, and, from personal experience, represent merely the tip of the iceberg.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
